
One of the most common questions I hear from patients starting medication-assisted treatment is: “How long will I need to be on this medication?”
They want a timeline. A finish line. A date when they can say they’re done.
I understand why. Most medical treatments have clear endpoints. You take antibiotics for 10 days. You wear a cast for six weeks. You complete chemotherapy in six months.
But opioid use disorder doesn’t work that way.
As Chief Medical Officer at CORAS Wellness, I’ve treated patients with opioid use disorder for over 17 years. I’ve learned that the question “how long will treatment take?” deserves an honest, nuanced answer, not a simple number.
Here’s what I tell my patients: We don’t have a limit.
That might sound discouraging at first. But understanding why there’s no set timeline—and what the actual trajectory of treatment looks like—can help you approach recovery with realistic expectations and patience.
The Chronic Disease Model of Substance use disorder
Let me start with something fundamental: opioid use disorder is a chronic medical condition.
Opioid use disorder is not different from high blood pressure, not different from diabetes. It is a medical condition that has to be treated.
Think about how we treat diabetes or hypertension. We don’t say, “Take this medication for six months and you’ll be cured.” We say, “This medication will help manage your condition. You might need it for years, maybe for life.”
Nobody questions whether someone with diabetes really needs insulin after five years. Nobody tells someone with high blood pressure that they’re taking the easy way out by staying on medication.
But with opioid use disorder, there’s still a persistent belief that real recovery means getting off medication as quickly as possible. That’s not supported by medical evidence, and it’s not how I practice medicine.
What I Tell Patients About Timeline Expectations
When someone asks me how long they’ll need to be on methadone or Suboxone, here’s my honest answer:
I tell them from the get-go, you’re going to be on this for a minimum of two to three years.
Notice I say “minimum.” For many patients, effective treatment lasts much longer.
Why two to three years? Because that’s the realistic timeframe for:
Stabilizing your brain chemistry
Long-term opioid use causes significant changes in your brain’s reward system, stress response, and impulse control. These changes don’t reverse overnight. It takes years for your brain to heal and relearn how to function without opioids.
Building a stable life
Recovery isn’t just about stopping drug use. It’s about building a life worth living. That means finding employment, repairing relationships, addressing legal issues, establishing housing, and developing healthy coping skills. This work takes time.
Developing new patterns
You need to establish new routines, new social connections, and new ways of handling stress. You need to experience holidays, birthdays, difficult seasons, and major life changes without using drugs. You need enough time to prove to yourself that you can handle life’s challenges while clean.
Addressing underlying issues
The trauma, mental health conditions, or circumstances that contributed to your drug use need treatment too. This work happens gradually through counseling and therapy, not on an accelerated timeline.
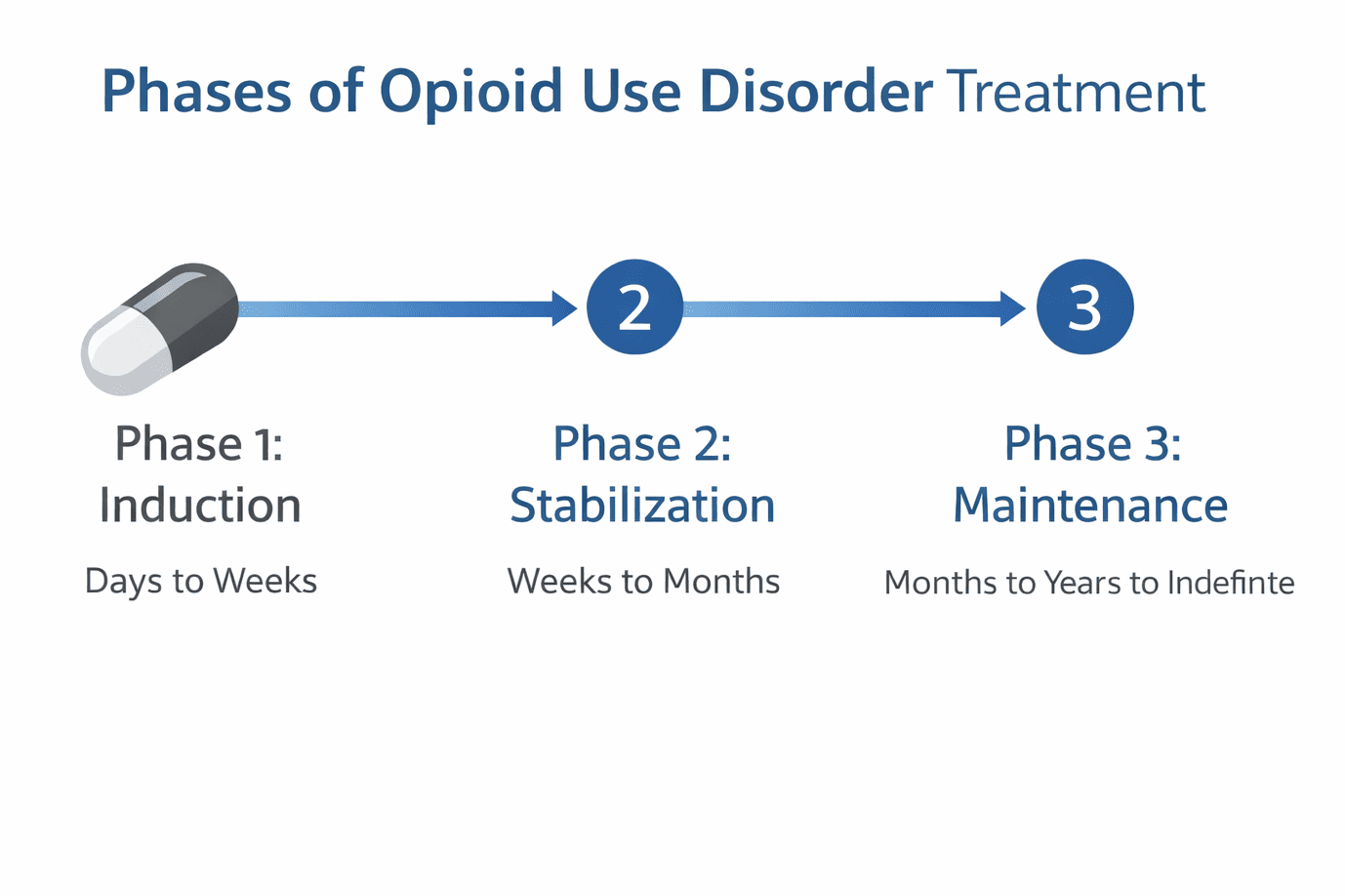
The Three Phases of Treatment
Medication-assisted treatment typically progresses through three phases: induction, stabilization, and maintenance.
Phase 1: Induction (Days to Weeks)
Induction is the initial phase when you start medication. The goal is finding the right dose to eliminate withdrawal symptoms and cravings.
For methadone:
We start at a low dose and increase relatively quickly to find your therapeutic level. We increase the dose rapidly to get you to a stable dose.
Most patients stabilize somewhere between 60 and 120 milligrams, though some do well at 20 milligrams and others need 150 milligrams or more. Everyone’s different.
You’ll come to one of our Delaware clinics in Dover, Newark, Harrington, Millsboro, or Wilmington daily during this phase.
For Suboxone:
You must be in withdrawal before taking your first dose. We then adjust the dose over several days to eliminate cravings and discomfort, typically reaching a stable dose of 16-24 milligrams.
The induction phase typically takes a few weeks. You’re not “in recovery” yet—you’re just getting stable enough to begin the real work.
Phase 2: Stabilization (Weeks to Months)
During stabilization, you’re on a consistent medication dose and you’re no longer experiencing cravings or withdrawal. This is when the real work of recovery begins.
This phase involves:
Regular counseling
Individual and group therapy become essential. The medication keeps you physically comfortable, but counseling addresses why you used drugs in the first place.
Developing new routines
You’re learning how to structure your days without drugs, how to handle stress, how to navigate relationships.
Addressing co-occurring issues
Mental health treatment, case management for housing or legal problems, rebuilding family relationships, finding employment.
Earning take-home privileges
For methadone patients, consistent negative drug screens and program compliance lead to take-home bottles, reducing the need for daily clinic visits.
The stabilization phase typically lasts several months. Some people stabilize quickly; others need a year or more.
Phase 3: Maintenance (Months to Years to Indefinite)
Maintenance is the long-term phase of treatment. You’re stable on medication, you’re engaged in counseling, and you’re rebuilding your life.
This phase can last: – Months for some patients – Years for many patients – Indefinitely for others
And that’s okay.
As long as the patient is productive, has a job, is taking care of their families, is not committing crimes, they can stay on it for as long as it’s necessary.
The goal isn’t to rush off medication. The goal is to live a productive, stable life.
Why There’s No Set Timeline
The honest answer to “how long will I need medication?” is: I don’t know.
Here’s why individual timelines vary so dramatically:
Everyone’s Brain Heals Differently
The severity and duration of your opioid use affects how long your brain needs to heal. Someone who used for one year will likely recover faster than someone who used for ten years.
The specific opioids matter too. Long-term fentanyl use might cause more severe brain changes than prescription opioid use.
Your age, overall health, genetics, and co-occurring mental health conditions all affect recovery speed.
Life Circumstances Vary
If you have stable housing, supportive family, and employment, you’re in a better position to focus on recovery than someone who’s homeless, isolated, and unemployed.
Some patients have significant legal issues that need resolution. Others are dealing with trauma that takes years to process.
Recovery happens faster when your life circumstances support it and slower when you’re constantly in crisis.
The Waxing and Waning Nature of Substance use disorder
Here’s something I see regularly in my practice:
Patients who’ve been stable for months or even a year or two sometimes relapse. They thought they were ready to come off medication. They tapered down or stopped entirely. And then life got hard, and they went back to using.
Some of them will stay off for maybe one or two years and then will come back. So it waxes and wanes.
This isn’t failure. This is the nature of a chronic relapsing condition.
The patients who come back are the smart ones. They recognize they need help again, and they get it.
The Process of Tapering Down
When a patient is ready to consider tapering off medication, the process must be slow and careful.
To come down we have to take it easy.
Why Slow Tapering Matters
If you’ve been on 120 milligrams of methadone for two years and you suddenly drop to 80 milligrams, your body will react badly. You’ll experience withdrawal symptoms, cravings will return, and relapse risk increases dramatically.
Instead, we reduce the dose gradually—perhaps by 5-10 milligrams every few weeks or months. Each reduction requires a stabilization period.
Each dose reduction requires the patient to get used to the new dose before we go down further.
This means tapering from 120 milligrams to zero could take a year or more.
The Psychological Component at Low Doses
Something interesting happens when patients get down to very low doses.
I’ve had patients that have not been able to get off one milligram of methadone.
At one milligram, the medication is doing almost nothing pharmacologically. But the patient is still getting something important from the program: structure, accountability, counseling, connection to the treatment team.
At that point it’s now psychological. They derive a lot of benefit in coming to the program, in the counseling.
And that’s perfectly fine. There’s no medal for getting off medication faster. The goal is stability and quality of life.
When Patients Want to Taper Too Soon
Sometimes patients push to taper before they’re ready.
Maybe they’re tired of coming to the clinic every day. Maybe family members are pressuring them. Maybe they believe they should be off medication by now.
I have these conversations regularly. And I’m direct about the risks.
Signs You’re Not Ready to Taper
You’re probably not ready to reduce your medication if:
You’re still experiencing cravings
If you’re thinking about using drugs regularly, your dose isn’t high enough yet. Tapering would make this worse.
Your life is unstable
If you’re dealing with major stressors like housing instability, legal problems, relationship crises, or job loss, now is not the time to reduce medication.
You’re not engaged in counseling
Medication provides physical stability, but without counseling to address the psychological aspects of substance use disorder, tapering is premature.
You have untreated mental health conditions
If you’re struggling with depression, anxiety, PTSD, or other mental health issues, these need to be stable before you consider tapering.
You’re testing positive for other substances
If you’re still using other drugs or alcohol, you’re not ready to reduce your medication.
The Danger of Premature Tapering
When patients taper too quickly or before they’re ready, I see predictable patterns:
They become uncomfortable. Cravings return. Anxiety increases. They start thinking about using “just once” to feel better.
Then they relapse. Sometimes they catch themselves early and come back to the clinic. Sometimes they spiral back into full-blown substance use disorder.
And here’s the frightening part: tolerance drops quickly after you stop using opioids regularly. If you relapse months or years after getting clean, the dose that used to be normal for you might now be fatal.
I’ve lost patients this way. They were doing well in treatment. They tapered off medication because they thought they were done. They relapsed. And the amount they used killed them.
This is why I’m cautious about tapering. It’s not that I want to keep people on medication forever. It’s that I want to keep them alive.
When Long-Term Maintenance Makes Sense
For some patients, staying on medication indefinitely is the right choice.
Who Benefits from Long-Term Maintenance?
People with severe, long-term opioid use disorder
If you used opioids heavily for many years, your brain might never fully return to its pre-disorder state. Medication allows you to function normally despite these changes.
People with chronic pain
Many patients developed opioid use disorder after legitimate pain treatment. Methadone provides both substance use disorder treatment and pain management.
People with multiple relapse attempts
If you’ve tried to get off medication several times and relapsed each time, long-term maintenance might be the safer option.
People with co-occurring mental health conditions
Conditions like severe depression, bipolar disorder, or PTSD can make maintaining sobriety without medication support extremely difficult.
What Success Looks Like on Long-Term Maintenance
I judge success by outcomes, not by whether someone is on or off medication.
Success means: – Stable employment – Healthy family relationships – No criminal activity – No use of street drugs – Management of mental health conditions – Overall quality of life
As long as the patient is productive, has a job, is taking care of their families, is not committing crimes, they can stay on it for as long as it’s necessary.
If you’re achieving these outcomes while on medication, that’s successful treatment.
Comparing Timelines: Methadone vs. Suboxone
Some patients choose Suboxone specifically because they believe it’s easier to taper off than methadone.
There’s some truth to this. Suboxone’s maximum dose is typically 24 milligrams, while methadone doses can go much higher. Mathematically, tapering from 24 milligrams is simpler than tapering from 150 milligrams.
But the timeline for successful treatment is similar regardless of which medication you’re on. Both require: – Time to stabilize – Time to address underlying issues – Time to build a new life – Slow, careful tapering when you’re ready
Don’t choose a medication solely based on which one you can get off faster. Choose based on which one works better for your individual situation.
Read more about Methadone vs. Suboxone here
The Role of Counseling in Timeline
The timeline for medication is closely connected to the timeline for counseling.
You have to start learning how to live a drug-free life. That’s where the counseling comes in.
Counseling and therapy help you:
- Process trauma and emotional pain
- Develop healthy coping skills
- Build new social connections
- Address co-occurring mental health issues
- Create a life that supports sobriety
This work can’t be rushed. You can’t process years of trauma in a few months. You can’t build a stable life overnight.
For some patients, our PHP/IOP program provides more intensive counseling support, especially early in treatment.
For others who need 24/7 structure and support, our inpatient drug rehab program provides residential treatment before transitioning to outpatient care.
What Happens If You Relapse?
Despite best efforts, some patients relapse after tapering off medication or leaving treatment.
This doesn’t mean you failed. This means you have a chronic relapsing condition that needs ongoing management.
Coming Back Is Strength, Not Weakness
When I see patients who’ve relapsed and returned to treatment, I don’t judge them. I welcome them back.
Some of them will stay off for maybe one or two years and then will come back. So it waxes and wanes.
The patients who come back are the ones who survive. The patients who don’t come back are the ones I worry about.
If you relapse, come back to treatment immediately. Don’t wait until things get worse. Don’t let shame keep you from getting help.
We’ll restart medication, readjust your dose, and work with you to understand what happened and how to prevent it next time.
How Other Health Conditions Are Managed: A Useful Comparison
When I explain long-term medication for opioid use disorder, I often compare it to other chronic conditions.
Diabetes:
Some people with Type 2 diabetes can eventually manage their condition through diet and exercise alone. Others need insulin for life. We don’t judge people who need insulin as “dependent” or weak.
Hypertension:
Some people can control high blood pressure through lifestyle changes. Others need medication indefinitely. Nobody questions whether they really need that blood pressure medication after ten years.
Depression:
Some people take antidepressants for a few months during a crisis. Others need them for years or decades to maintain stability. This is accepted as appropriate medical treatment.
Opioid use disorder works the same way. Some people need medication for a few years. Others need it longer. Both are legitimate, evidence-based approaches to managing a chronic condition.
Common Questions About Treatment Duration
What if I need to be on medication for life?
Then you’ll be on medication for life, and that’s okay. The alternative—active substance use disorder or death from overdose—is far worse.
Will insurance keep covering my treatment?
Most insurance plans, including Medicaid and Medicare, cover medication-assisted treatment for as long as it’s medically necessary. There’s no arbitrary cutoff.
What will people think?
I understand this concern. There’s stigma around medication-assisted treatment.
But here’s what I tell patients: Would you rather be judged for taking medication while living a productive life, or would you rather be using street drugs?
The people who matter will understand that you’re getting medical treatment for a medical condition. The people who don’t understand aren’t the ones whose opinions should guide your healthcare decisions.
Can I have a normal life while on medication?
Absolutely. Most of my patients work full-time, raise children, maintain relationships, and pursue goals.
Our methadone clinics open at 5:00 a.m. specifically so patients can dose before work. As you earn take-home privileges, you’ll spend even less time at the clinic.
Medication doesn’t prevent you from living a normal life. Active substance use disorder does.
The Bottom Line: Focus on Quality of Life, Not Timeline
The question “how long will treatment take?” assumes there’s a finish line where you’re “cured” and done.
But opioid use disorder doesn’t work that way. It’s a chronic condition that requires ongoing management.
The better question is: “Am I living the life I want to live?”
If medication-assisted treatment, combined with counseling and support, helps you: – Stay off street drugs – Maintain employment – Repair relationships – Manage mental health – Stay out of legal trouble – Feel like yourself again
Then treatment is working, regardless of how long you’ve been on it.
I’ve seen patients transform their lives through comprehensive treatment. I’ve seen people who were homeless get housing. I’ve seen people who’d been in and out of jail for years stay clean and free. I’ve seen parents regain custody of their children.
These outcomes don’t happen on a predetermined timeline. They happen when patients commit to treatment, engage with counseling, and give themselves the time they need to heal.
What Makes My Work Worthwhile
After 17 years of treating patients with opioid use disorder, what keeps me going are moments like this:
When somebody tells me, “Thank you, doctor. I feel so much better. I have a job now. I’ve gotten my children back,” there’s nothing that feels better than that.
These transformations don’t happen in three months. They happen over years of committed work.
But they do happen. And they’re worth the time it takes.
Ready to Start Treatment?
At CORAS Wellness, we provide comprehensive medication-assisted treatment without arbitrary timelines or pressure to taper before you’re ready.
Our approach includes: – Medical care from board-certified substance use disorder specialists – Individual and group counseling – Mental health treatment for co-occurring conditions – Case management for housing, legal, and employment issues – Flexible treatment that adjusts to your individual needs
We serve patients across Delaware at our locations in Dover, Newark, Harrington, Millsboro, and Wilmington.
📞 Call 833-886-2277 to speak with our treatment team and learn about our comprehensive approach to opioid use disorder.
Treatment works. Recovery is possible. And you deserve care that’s focused on your wellbeing, not on rushing you off medication.
If you’re struggling with other substance use issues, we also offer specialized programs including our DUI and Alcohol Education Program.
About Dr. Okechukwu Ernest Obua
Dr. Okechukwu Ernest Obua serves as Chief Medical Officer at CORAS Wellness & Behavioral Health, where he oversees medical care for all patients across the organization’s methadone, detox, and rehabilitation programs.
Dr. Obua trained in family medicine at Henry Ford Hospital in Detroit, where he developed a deep interest in addiction medicine after witnessing the confusion and inconsistency in how opioid prescriptions were handled. Since completing his residency in 2009, Dr. Obua has practiced addiction medicine exclusively, specializing in running methadone clinics as a medical director.
Dr. Obua holds the following board certifications and credentials:
- Diplomate, American Board of Family Medicine
- Diplomate, American Board of Addiction Medicine
- Diplomate, American Board of Preventive Medicine (Addiction)
- Fellow, American Society of Addiction Medicine (FASAM)
He attends the annual ASAM conference to stay current on new developments in addiction treatment and evidence-based practices.
His approach to treatment timelines is grounded in medical evidence and compassion. We don’t have a limit. As long as the patient is productive, has a job, is taking care of their families, is not committing crimes, they can stay on it for as long as it’s necessary. This philosophy recognizes opioid use disorder as a chronic condition requiring individualized care rather than arbitrary deadlines.
With more than 17 years of experience in addiction medicine and a deep commitment to his patients, Dr. Obua brings both clinical expertise and genuine care to his work at CORAS Wellness.